In the latest of our quarterly updates, we use our unique, national dataset to look at the key trends in the independent healthcare sector up to, and including, Q2 2024. The data covers private healthcare in-patient/day-case market activity, insured cases, ‘self-pay’, along with national/regional and procedural breakdowns and demographic information. (Q1 = Jan – Mar; Q2 = Apr – Jun; Q3 = Jul – Sep; Q4 Oct – Dec)
Private healthcare sector market activity
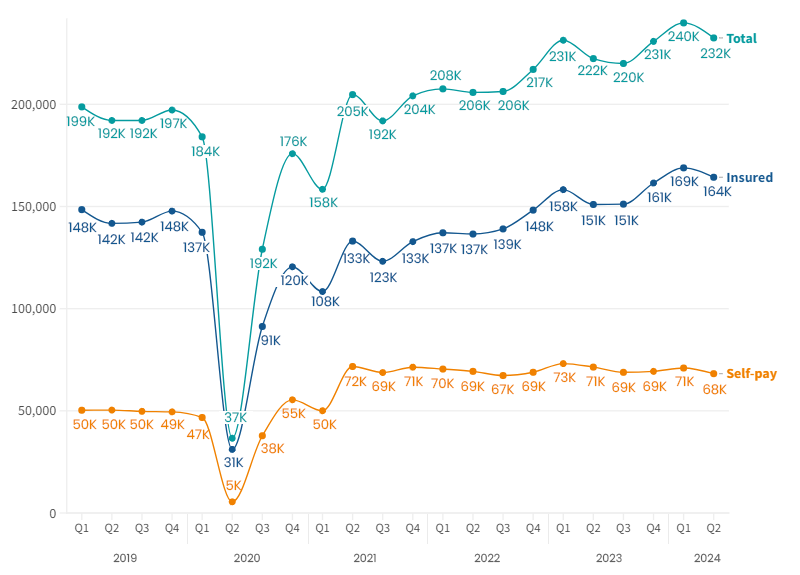
In-patient/day-care admissions comparison Q1 2019 – Q2 2024
Q2 2024 at a glance
- Highest ever reported private hospital admissions for a second quarter (Apr-Jun)
- Second highest total admissions on record, up 5% on Q2 2023
- Private medical insurance (PMI) up 9% on same quarter in 2023
- Self-pay remains steady, but 5% down on same quarter in 2023
- Reduction in reported admissions for several cosmetic procedures
- Robot-assisted procedures continue to increase
Independent healthcare in-patient admissions in Q2 2024
There were 232,000 admissions in Q2 2024, a 5% increase the same period in 2023.
There was a small decrease in admissions (3%) from Q1 2024, but this follows an established seasonal pattern. The total admissions, as well as those paid for with private medical insurance, were at the second highest ever level (after Q1 2024).
The gap in admissions between those paying with PMI and those using ‘self-pay’ was up to 96,000 from 80,000 in Q2 2023.
Self-pay has consistently been more popular than it was before the pandemic and remains 36% above pre-pandemic levels, despite a small decline.
Admission change (%) by Nation (Q2 2023 v Q2 2024)
%20by%20Nation%20(Q2%202023%20v%20Q2%202024).png)
Northern Ireland had by far the largest increase in reported hospital admissions. This could be in-part due to improved reporting from the hospitals in that country.
England had the smallest level of growth, but has the highest volumes of admissions. There was an increase in admissions in every English region except the South East (-0.3%), and Yorkshire and The Humber (-1.2%) which had very small decreases.
Admissions by English Region and payment method (rounded figures) (Q2 2023 v Q2 2024)
.png)
Private medical insurance admissions continue to grow as self-pay remains steady
Insured admissions
When comparing Q2 2024 to Q2 2023, the number of admissions funded by private medical insurance rose in every English region, except the South East and North East. The North East continued to have the fewest insured admissions (2,000) in these quarters.
London once again had the most insured admissions (rising from 54,000 to 61,000), followed by the South East (29,000).
Insured admissions were also up in Northern Ireland and Scotland, but did not change significantly in Wales.
Self-pay admissions
Self-pay fell in London, the South East and South West comparing Q1 2024 to Q1 2023. The was no significant change in the other English regions or devolved nations.
Insured and Self-pay change (%) by Nation (Q2 2023 v Q2 2024) (based on non-rounded figures)
%20by%20Nation%20(Q2%202023%20v%20Q2%202024).png)
Top 10 procedures (Q2 2023 v Q2 2024)
.png)
There was an increased number of episodes in eight of the top 10 procedures by volume when comparing Q2 2023 and Q2 2024. Therapeutics – chemotherapy had the largest increase (17%).
Although the above graph appears to show a decrease in both Hip replacement (primary) and Knee replacement (primary). We now report those procedures separately for without robot-assistance and with. Once the assisted surgery is included, there is 4% reduction in hip replacements and a less than 1% change in the number of knee replacements from Q2 2023.
Robot-assisted hip replacements were up 53% (590) and knee replacements were up 58% (790), see our report A helping hand for more information on this type of assisted surgery.
Outside the Top 10 procedures, breast lifts (-18%), enlargements (-7%) and reductions (-9%) were all down from Q2 2023, as were face lifts (-16%) and weight loss bypass surgery (-20%) and weight loss gastrectomy surgery (-23%) and tummy tucks (-18%). These are all often cosmetic procedures which aren’t usually available on the NHS or through PMI.
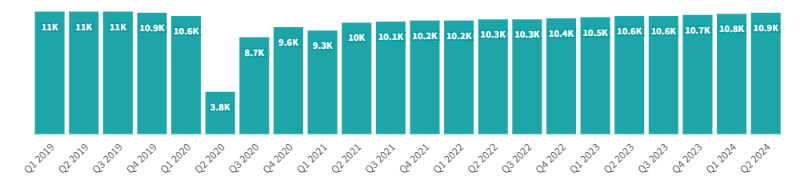
Active consultants in private healthcare (Q1 2019 - Q2 2024)
Quarterly comparison of active consultants for the top 10 PHIN specialties (Q2 2023 v Q2 2024)
.png)
The largest increase in active consultants in the top 10 procedure groups was in ‘Clinical oncology’ had the second largest increase in volume (an extra 26 consultants) and the largest percentage increase (14.5%).
‘Medical oncology’ was the only specialty in the Top 10 that had a reduction in the number of active consultants with 4 fewer (-1%).
Patient demographics
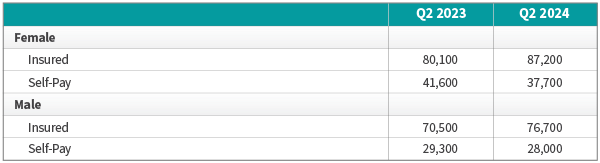
Volume of admissions by sex and payment method (Q1 2023 v Q1 2024)
There was an increased number of insured admissions and reduction in self-paid admissions for both sexes compared to the same quarter in 2023.
The growth in insured admissions for males was 6,200 (8.8%) compared to 7,200 (8.9%) for females.
The drop in self-pay was also at a similar level for male admissions at 1,300 (-4.4%) compared to 1,900 (-4.5%) for females.
Admissions for females continue to be higher than for males across both payment methods.
Purchaser type and sex (Q1 2023 v Q1 2024)
Change in volume of admissions by age
Admissions in all age groups up to and including 60-69 year-olds increased when comparing Q2 2023 and Q2 2024. The largest increase by volume and percentage came in the 10-19 year-old age group.
There was a decrease in admissions for the 70-79 and 90-99 year old age groups. The rest all increased.
.png)
Comparing Q2 2023 and Q2 2024, the use of insurance to pay for admissions was up in every age group. The largest increase by volume was in the 40-49 year-old group. The largest percentage increase (16%) was in the 10-19 year old group.
In contrast, the use of self-pay reduced in every age group except 10-19 year-olds where there was a slight (1%) increase. The largest decrease by volume came in the 70-79 year-old group (-810) and the largest percentage decrease was for 90-99 year-olds (13%).
Important notes
All data described above taken from PHIN’s unique, national private dataset describing discharge activity (day case and inpatient). This excludes activity outside of PHIN’s mandate from the Competition and Markets Authority, such as outpatient diagnostics and mental health.
There is a time lag between collecting, validating and processing the data we receive from hospitals before we can publish it. This can be up to 6 months after treatment has been completed, to ensure a fair process and accurate data.
Activity numbers have been rounded to the nearest 5, with percentage based on the unrounded figures.
